

Blog posts on Nourished Waters
What does pain in labor have to teach us?
My fourth baby was the most painful... despite everything I know, I still had a ton of body issues which resulted in the only truly painful birth I've had...
The thing I feel most important to share about this is that I FULLY grokked how to transcend pain in labor. I'd had 3 prior births that were pain transcendent...3 beautiful, instinctual, primal births, 2 without assistance.
But my 4th baby, (another freebirth) born just 3 years almost exactly after her brother, would not stay in an anterior position no matter what I did (and I know all the ways... she would turn but not stay).
She was not only hanging out posterior through the end of pregnancy and likely into labor, but she also dropped VERY early... like months early.
The result was a ton of inflammation in my pelvis- and that includes in those pelvic nerves- contributing to pain in pregnancy, and in labor.
But why would this happen?
Well, I had my reasons...
I struggled a TON in pregnancy with getting exercise. My body was having a lot of difficulty with the progesterone surge and blood volume increase.
The disease I've struggled with for over 24 years, Lyme, was flaring. My body hurt. I was exhausted. I didn't want to admit I was flaring, but it's likely.
And, my old injuries to my sacrum and general ligament issues from years of Lyme damage, all coalesce into a really not fun experience of pregnancy.
I do my best- but pregnancy is definitely not my friend (and I'm so grateful for the end result- I just don't love the pain and extreme Yin fatigue of pregnancy).
My pelvic floor was imbalanced and weakened in such a way that my body simply could not hold my baby up any more. She dropped deep, her head grinding into those pelvic nerves, and favoring that posterior position, which likely had to rectify in labor itself.
I share this because I recognize how hard it is to do the things that we know would help, even when we know them.
And, there is so much information overload out there...
I also know that some of us struggle with more body issues than others... which is why we need tailored, easy, QUICK self-care regimens that don't wear us out or overstrain an already strained body.
What we need to understand is that the body and pelvic floor are more than just a set of rules that physiology should follow… they are living, breathing, complex interplays between muscle, bone, nerve, fascia, and so on, which respond to hydration, to pressure, to neurology and hormone, and so much more…
We need to learn how to care for our bodies in this modern era. We have become so stagnant, so disconnected from our source, from our Earth, from our natural foods and ways of moving and breathing, that things which once did happen relatively easily for us (and still do for indigenous people) now have become supposed cause for a nearly 50% C-section rate in America (of course we know a lot of this is also fear-mongering and capitalism).
But my point is… our bodies WERE made for this, but as we move, grow, develop and create habitual patterns in our bodies, including stress patterns of tension and misuse patterns of weakness, our bodies have become less resilient, less capable of holding that strain in a good way…
And it’s both not our fault, and yet still our responsibility, to learn better.
We do have to actively work to re-wire our neurology, our patterns of movement, even our breathing, to find balance again.
My pelvic floor had become weak in some areas, and tense in others, due to a combination of factors both in my control and not. Lyme damage, sacroiliac injury 17 years ago, ligament laxity as a result… having had a prior baby more recently… chronic constipation during this pregnancy, and a lack of exercise and healthy movement patterns due to some of the above and other physical factors… all contributed to that baby just not wanting to leave the posterior position, and dropping into my pelvis early IN that posterior position… further compounding my constipation issues, my pelvic floor issues, my ligament strain, and my pain…
Our NERVES are the seat of the pain in our labors (or Pleasure!!)… and it is those nerves that we need to tend to, through tending to the musculature around them. There really is a lot I could have, should have, would have done even prior to that pregnancy to prevent these later issues… and had I the time, energy, and health, I would have.
I certainly forgive myself, but I also somewhat kick myself for not being a little more proactive, trying just a LITTLE harder to get my butt (literally) in gear during that pregnancy. Because the truth is, there probably is a lot I could have done even with some of the more basic exercises I know to do… but I also wasn’t even the expert then as I am now (despite 14 years of working with neuro-structural bodywork, now I am an expert in corrective exercise for prenatal and postpartum too, which is a whole new level of understanding.)
I'm developing my map for you all, and slowly trickling that information onto the birth education app, Nourished Waters Birth Portal, so that pregnancy AND postpartum recovery can be simplified and accessible to you, even if you feel utterly overwhelmed with the idea of exercising in pregnancy.
I also cover a lot of valuable information on this in my book, The Myth of Pain-Free Birth. Link to buy is on my home page.
What do you wish that you knew then or even now, that could help your body better prepare for birth, or recover after?
Let's talk about it. :)
What do you wish that you knew then or even now, that could help your body better prepare for birth, or recover after?
Let's talk about it.
What is Fetal Ejection Reflex (FER) and what does it have to do with my Pelvic Floor?
My body pushed my babies out involuntarily.
I didn’t push. At all.
Not only that, but for all four of my births I didn’t tear at all, AND I experienced transcendence of pain in all but one birth (and I know why that one was different… and I’ll share it with you!).
I’m sharing this because I truly believe that when birth is left alone, most womben will actually experience this, and furthermore, with a healthy pelvic floor, they may experience this as I did, with minimal pain, and instead in a state of euphoria.
What is Fetal Ejection Reflex (FER)?
And what does it have to do with my pelvic floor neurology?
FER, also known as the Ferguson reflex, in simple terms, is when the body involuntarily bears down to push the baby out during the second stage of labor, rather than having to intentionally push.
Typically what happens here is that the body, sensing the baby’s head or other presenting part pressing on the pelvic nerves, sends a signal to the brain which causes a release of oxytocin, causing some big contractions. It also sends a surge of adrenaline to mother and baby, bringing the laboring woman out of the endorphin rich “la-la labor land” that she was in during first stage and likely in the pause between first and second stage (the quietude). This causes the womban to feel the urge to get more upright, alert, and ready for being fully present as the baby emerges.
Our uterus has receptors in it for the hormone oxytocin, the hormone which many know of as the hormone of love and bonding, and, miraculously, also is the hormone responsible for uterine contractions! In late pregnancy, the uterine oxytocin receptors increase around 200x!
But what we need to understand is that there is a feedback loop between the brain and the pelvic and cervical nerves which causes the brain to release more oxytocin as well as other hormones, when the fetal head (or other presenting part) puts more pressure on those muscles and nerves, and stretch receptors of the cervix itself.
The cervix is the star of the show in the first stage of labor, and those stretch receptors are largely responsible for the signal to the brain to release more oxytocin, causing stronger contractions, which in turn helps bring that lower uterine segment up to build the fundus, opening the cervix more.
But in the second stage of labor, the star of the show is actually the pelvic floor, and specifically the nerves within that sling of muscles, and on the interior surface of the sacrum. We have to remember and understand that muscles respond to stimuli, meaning pressure sensation, on the nerves with contraction or relaxation.
We also must understand that there are several types of nerves, relating to the central (sensory) and autonomic (sympathetic and parasympathetic) nervous system. Each of these have a unique function and effects on the hormonal response in the brain.
Additionally, every womban is going to have slightly different nerve pathways, as we all have variations in our anatomy. So no womban will have the same experience of pleasure or pain in her pelvic area.
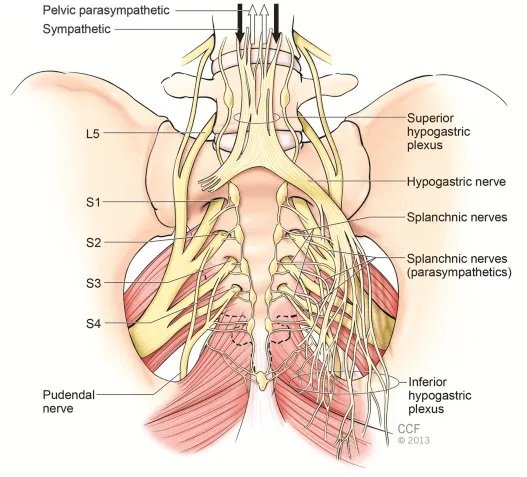
The primary nerves of the pelvis that are the stars of this show, are the pudendal nerves, which are mixed sympathetic, motor and sensory nerve fibers that wrap around the perineum, anus, and clitoris, and the pelvic splanchnic nerves which are parasympathetic fibers that emerge from the interior of the sacrum, as well as the sacral sympathetic splanchnic fibers.

When our body has finished pulling up the lower uterine segment, also known as “cervical dilation”, the baby either immediately or soon after drops down to the level of the ischial spines. At this point, there is a very important, often overlooked, cardinal movement that the baby makes, again sometimes instantly, sometimes after hours of pause. This is the internal rotation of the head to clear the ischial spines, letting the head through this narrow landmark in the middle of the pelvis, allowing it to then fully drop to meet the pelvic floor musculature and nerves, and the perineum, for crowning.
Here is a look from below at this bony landmark. Do you see the points facing inward? These are the ischial spines. Can you see how it would be hard for the baby’s head to go further in this position? This is why we need this moment of pause called the Quietude or Rest and Be Thankful stage after dilation, and before “pushing”, to allow the baby to navigate this landmark and drop fully.

“The second stage is defined as the stage when the cervical dilatation is full. However, the second stage diagnosis must include the fetal head position at ischial spine at level zero according the ACOG classification. The diagnosis of fetal head (FH) position in the birth canal is performed by traditional vaginal digital examination (VE) and recently by intrapartum ultrasound (IU) also. The diagnosis of second stage based only on cervical dilatation is incomplete and requires the diagnosis of FH in the birth canal.” (1)
This is a really important distinction to understand, and while this may seem like a very dense subject so far, I want you to have enough understanding of your anatomy and the physiology of birth to be able to understand the following point:
If we begin pushing just because a womban is fully dilated, rather than confirming that the baby is not only at the “zero station” at the ischial spines, but actually that the baby’s head has rotated to get past the ischial spines, we are making a grave mistake. The result is that a womban may push and push and push for long hours, while the baby remains stuck on those spines, unable to rotate and drop fully down into the pelvic floor.
We also may find that the act itself of pushing before the Fetal Ejection Reflex kicks in, may override the sensitive neurological signals coming from the nerves of the pelvic floor.
Here is the main point I want every birthing person to understand:
A healthy fetal ejection reflex is going to be more achievable if we create the right environment. It is long understood from the experiments done by Constance Benyon and Michel Odent that if we give womben enough time, most will end up having a physiologically self-directed pushing stage, perhaps even with a strong FER.
Even in the following research in 2004 and 2020 we found an important correlation between a woman feeling safe in labor, and the hormone cascade. If a womban feels scared, threatened, or the environment simply doesn’t foster peace, the body will send stress hormone catecholamine, which will slow down the labor and inhibit FER even in a healthy womban. (2)(3)
Fostering an environment of safety, non-disturbance, and patience is crucial.
What I think is missing from some of this earlier research is that we also need to consider some of the other factors at play in individual womben’s anatomy.
Our pelvic floor function is going to be individual to our unique body and life experience. In our current paradigm, most of us spend more time sitting than we are designed for, and historically, indigenous humans have spent more time walking, squatting, and changing activities throughout their day. This alone is going to change how our body behaves, and how our pelvic and other muscles work.
Then there are additional factors such as tailbone traumas, other accidents or injuries, excessive weakness due to lifestyle factors, inflammation or even simple muscular imbalances due to imbalanced movement patterns in life or workouts.
These imbalances can cause muscles to become weak on one side, and tense on another. They can cause impingement of nerves within muscle fibers that have been caught in tension patterns. Muscles can also be both tight and weak at the same time, because that tension pattern prevents them from contracting or releasing fully. And all of these factors can contribute to inflammation in the muscle and nerves.
The result in these cases is the potential for more pain in labor, as well as potentially causing the baby to descend in an imbalanced manner, putting undue stress on one side or another, and on the nerves in a particular part of the pelvis. Even a tight psoas muscle on one side may be a factor in the way the baby lays in the uterus and descends into the birth canal.
And, when the baby drops into the nerve-rich musculature of the pelvic floor, including onto the sacrum with its interior covered in nerves, including the parasympathetic splanchnic nerves, this pressure, when evenly applied to a healthy, unobstructed nervous system, can cause the cascade we call the Fetal Ejection Reflex.
The parasympathetic and sympathetic nerves receive this pressure sensation, sending signals to the brain to both open and relax, while also creating a surge of oxytocin and adrenaline for a series of profoundly strong contractions which cause this immense, involuntary bearing down sensation.
It is my clinical hypothesis, which I have witnessed in my work as a bodyworker, that impingement on these nerves due to tailbone, pelvic floor or sacral traumas and imbalances, can augment this FER. This may potentially inhibit a healthy nerve response, interrupting that potential cascade leading to FER, and oftentimes also correlating with increased pain.
But I’m not going to leave you hanging here!
There are very profoundly helpful things you can do to ensure a healthy pelvic response prior to or during pregnancy.
A combination of pelvic floor release work done either at home (as I teach in my online courses) or by a professional, along with pelvic floor physical therapy as needed for a tailored approach, and/or pelvic floor and general exercises like I teach in my program, can go a long way to ensuring we enter the birthing tides in balance. We need to be able to address areas of tension and holding patterns first, and then look at how we move, breathe, and exercise, second. This combined approach is, in my opinion, the core of childbirth preparation which needs to be given more consideration in our modern era.
I am doing my best to address this gap in our education, one person at a time. To learn more, and delve deeper into this subject and my expertise on this, visit https://nourishedwatersbirth.com and join my cohort of amazing womben learning all about their bodies and babies in the birth and postpartum continuum. Even if you have had a history of painful labors, long second stage, or trauma, you can take action here and now to heal, recover, and potentially prepare for another baby in the best way possible. I hope to see you there!
1.) Antonio Malvasi et al. Oxytocin augmentation and neurotransmitters in prolonged delivery: An experimental appraisal. European Journal of Obstetrics & Gynecology and Reproductive Biology. March 2024. Available online at https://www.sciencedirect.com/science/article/pii/S2590161323000996
2.) Ibone Olza et al. Birth as a neuro-psycho-social event: An integrative model of maternal experiences and their relation to neurohormonal events during childbirth. PubMed 2020. Available online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386571/
3.) Judith A Lothian, Do Not Disturb: The Importance of Privacy in Labor; PubMed 2004. Available online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1595201/
Interference in the Birth Room... the Wise Midwife
The Wise Midwife Performs Her Work By Doing Nothing…
Women go to a midwife, choose a home or birth center birth, most often because they believe they will be receiving a different type of care. We may have had a past trauma in a hospital, or may have an instinctual knowing that the hospital is not the place we want to have our first baby… and so we seek what we believe is the most “natural”, and woman-centered care provider we can find.
I have been a student midwife, doula, and birth attendant as well as home birth/free birthing mother, for over 16 years now, and I can tell you one thing I have noticed and realized in talking with other womben, both mothers and birth workers:
Midwifery isn’t always better.
There is a whole political landscape I could let you in on here, and a lot I could say about the way in which licensure and the medical model, as well as laws which do not protect home birthing families’ true rights and autonomy, plays into this. But instead of getting super politically charged right off with you, I want to speak to something deeper… In other words, rather than revealing the reasons I believe this is happening, I want to speak to what is happening first, because I do believe that midwives and other birth attendants have more ability to bring greater self-reflection and better practices into their repertoire NOW, rather than assuming that we have no choice in the matter.
I will never forget my second child’s birth. Laila was born at home, in the water, with a midwife and her apprentice present, in addition to my partner and older son ‘Io who was 7 at the time. It was four hours from the first real contraction and breaking of my water, until birth.
I had, as you may know by now, an unintended free birth with my first child. But this time I still believed having a midwife was best, and I had been a midwifery apprentice in the time between my first and second baby. I chose a woman who I felt was one of the more experienced midwives in the area, with over 30 years under her belt. I talked to them about my desire for autonomy, and they agreed it was a reasonable request. I thought we were on the same page.
But then, they arrived. Immediately, my sweet, candle lit environment was lit by the overhead light. I “negotiated” for the dimmer switch to be employed to turn it down, but she insisted some light was necessary (beyond 20 candles?) to take notes and so on. Being in hard labor already, I didn’t feel like I had the bandwidth, and frankly the guts at that stage in my life, to insist otherwise.
Meanwhile, they sat in the other room as I requested, whispering away. And then came time for some of the last centimeters dilation, the transition… and I felt a bit stuck. Everything about the presence of the midwives felt invasive, even that which was relatively benign… because I had experienced the exact opposite with my first birth, where no one was there except my partner, and I was able to labor through in the dark with zero distractions.
They didn’t mean to disrupt, but they also did. I checked my own cervix, and found myself with a little lip of cervix left. My mistake, if you will, was that I told the midwife what I discovered. Out came the homeopathics, a relatively gentle medicine, but still effective to a degree which increased my contractions to a level that was unnaturally strong feeling.
And then I let it be, as I knew my body would figure it out. I waited, felt the head begin to come out, felt it recede… I was much too in my head and actively trying to let her know what was happening while she looked on from the side, watching every movement… She urged me to push, and so I did a little. Thankfully, my body did the rest, and fetal ejection reflex kicked in, bringing her out swiftly just as with my other babies. Little harm done, right? I didn’t tear. Everything seemed fine, despite my feeling a little annoyed that it wasn’t a more quiet, dark, private birth room.
But then a bit under a week later I developed a big, painfully swollen hematoma in my vaginal wall. There are of course many possibilities of why this could have happened but I couldn’t help but feel as if it wouldn’t have happened had I been left alone, without the unusually strong contractions and coached pushes…
I recognize my part in the midwife’s choices. Had I not worried about the cervical lip, they may not have given me the homeopathics… But here’s the thing: the midwife herself has two choices in any situation. She can feed the fear, or feed the calm.
In a four hour, otherwise absolutely normally progressing labor, there is no reason why a cervical lip should be seen as anything other than a mama needing a bit more time to work through that last bit of dilation. It was posing no problem. I was in my head, because in retrospect, those around me were in their heads.
Those in the room with a laboring mother, may serve best from a place of being able to drop into deep, meditative presence, fully aware still, but in a deeper brainwave state more compatible with that of the laboring mother who is entering an altered state. Being in your own monkey mind, has the inevitable effect of entraining the mother’s brainwaves to your own, bringing her out of that altered state and into a Beta thinking brain herself.
Beyond this, of course, I have a plethora of things to say about the subtle and not so subtle ways that birth attendants mess with the vibe that allows women to drop deeper, and find their animal body instincts. Too much light, sound, asking questions, hovering over, touching, giving medicines, or otherwise imposing one’s own will and needs on the birth space, inevitably has the result of bringing a woman out of Delta or Theta brainwaves, and back up to the Beta brain.
Every single action and word we take must be weighed against the potential it has for interference and distraction of the mother from her deep dive into her own center.
Any action we take has the potential to move the woman’s locus of power, her Center, from within her, to us. As I noticed with my own midwife-assisted birth, my sense of needing to inform the midwife, through my own vaginal exams, or as most women would experience, through the midwife’s exams, brings the focus away from our deep inner landscape in the veil between worlds, and into the realm of the “living”. Beta brain.
Beyond just distracting, there are also infinite ways that well-meaning doulas and midwives impose their own will on the birthing mother, rather than asking themselves if it is even necessary. Or, as in the case of needing lights on to take notes, is there any other way that I can get my needs met that does not impose my will on the birthing mother?
Any time we find ourselves asking a mom or dad to do a certain thing, or Goddess forgive, doing something to the laboring womban, we are imposing our will upon them.
That isn’t to say that there is never a time or way to suggest things, but it is definitely best to keep clear communication with a focus on suggestion rather than telling or even asking. In other words, we ask for consent, and give gentle ideas if a womban asks for help… and even then I ask myself, does she really need my guidance or words right now, or does she need me to simply tell her, even wordlessly, that she is exactly where she needs to be?
I sincerely believe that most womben, if we just calmly remind them that there is nowhere but here, and now, and that they’re doing it, will find that extra reserve to dig deeper into and find the answer they are seeking, without my guidance at all!
This requires of us a deep sense of wonder, awe, reverence for the birth process… as well as deep trust that womben are capable of undisturbed, instinctual birth.
It also, of course, requires that we put down any egotistical need to be involved, both from the vantage of wanting to stroke our own ego, as well as more subtly feeling the need to justify our being there. If I find myself wondering why I am there, rather than try to find a way to act in order to justify it, perhaps it’s a sign I ought to sit on my hands even more, or leave the room entirely, so the laboring womban can dig deeper.
Perhaps the need to check the baby comes not from a sense of care for the welfare of the baby, but from a deeper sense of needing to be busy, active, and useful in a situation which is inevitably rarely actually going to call upon our deepest midwifery faculties. Are we sure that we need to be checking on the baby or the cervix, or is this just something we have become accustomed to the redundancy of, and have forgotten the sacredness and potential for interference of each of these actions?
This calls us to reveal a deeper capacity to be with womben… to step into a place of reverential containment, into our own spiritual root which allows us to enter a meditative, wordless state, from which intuition of our own can arise. We have to be willing to allow and accept that a womban ultimately is the authority of her own birth experience, and only she knows exactly how she needs to move, position herself, intonate, and so on to get that baby out.
Our expertise may come in handy if she is truly stuck, needing help, or experiencing an emergency… but even in an emergency, it may actually be moreso the way in which we handle a situation, rather than the actual skills used, which help resolve the issue. This is something I will get into more deeply in another article, perhaps.
So, as a womban having a baby, how do you find a provider who understands this nuance, and is not simply going to manipulate your birth experience to her own ideologies, legal parameters, and personal needs and ego?
This is something I delve into in depth, in great detail, in my free resources, particularly the Choosing Your Birth Attendant workbook. You have a lot to think about in pregnancy, and it can be very overwhelming trying to figure out what questions to even ask. That’s why I’ve created these resources… to help you ask the questions you didn’t even know to ask, and begin to curate your own birth blueprint as well as finding the provider that is right for you.
You can find this free resource on my Free Resources Portal at https://nourishedwatersbirth.com

Is Every Woman Capable of Experiencing Fetal Ejection Reflex (FER)? ~ “Breathing Your Baby Out”
Whenever womben “should” one another, I internally cringe. There is so much anti-ideological ideology in the world… its’ dizzying. There is the die-hard “hospital birth is the only safe option” crowd… but then on the other end of the spectrum, there is just as much ideology, some of which actually may be just as harmful, and certainly can give some false security.
Women have been speaking a lot on social media, etc about Fetal Ejection Reflex (FER), and what some call “breathing your baby down”. It’s become a hot topic, and there are inevitably many opinions on the subject, some who say it is the luck of the draw, others who say that every woman “should” wait until they experience this. What the heck is real?
Well, as a long time pelvic floor care bodyworker turned doula /birth tender, I can honestly say there is a lot more to the picture than meets the eye.
I myself experienced FER with all four of my babies’ births. To me, it was in most of those births, a freight train that if anything, I had to breathe and focus to slow it down to allow my tissues to stretch and not tear. I never needed to push, and aside from my one birth with a midwife, who told me to try pushing when I really didn’t need to, I didn’t. Even then, once the baby truly reached my pelvic floor, there was no stopping it, and no need for focused pushing. My body essentially does it on its own.
But I am certainly aware this is not the experience of every woman. For some, however, the “pushing” stage (second stage of labor) is excruciatingly long, and for that, I have to question, are we having her push too soon?
The answer in most hospital settings, and even some home birth settings as I saw even with my own “extremely experienced” midwife, is that we typically are not waiting long enough. Michel Odent, and before him, Constance Benyon, did extensive experimentation with stepping back from the role of “coach” in labor, instead waiting to see how often women would have the spontaneous urge to push, or better yet, Fetal Ejection Reflex.
I place these two in slightly separate categories, though the line is truly blurred, only to highlight the fact that for some women this FER sensation will be felt as the need to push, a deep, bodily sensation accompanied by an almost involuntary but wholly satisfying bearing down. For other women, and I would say I generally fall into this category, the body does the bearing down entirely on its own without even having a sense of desire to push… perhaps it is only a matter of timing in these cases, that the urge and actual bearing down impulse are so instantaneous and so strong, that there is absolutely no conscious sense of pushing on the womban’s part. Or, perhaps there is a bit more nuance there between the woman who feels the FER but still has a need to consciously push with the urge, versus the woman who’s body does the pushing for her entirely involuntarily.
Either way, it seems that once this happens, there is almost no stopping. The body takes over, the urge and even satisfaction of bearing down far outweighs any desire not to.
We have to understand, and I speak about this in great depth in my online and local classes, that many doctors and even midwives will coach a womban to push immediately when she reaches 10 cm dilated. Some even tell a womban to push before she is fully dilated!
This is, in my humble but educated opinion, extremely dangerous and detrimental to the natural and healthy, safe physiologic unfolding of the birth process. The baby is still at the ischial spines when dilation is occurring or has just occurred, and the baby’s head must make an internal rotation to clear the ischial spines properly, and for the head to emerge in a different angle than the rest of the body. If we push too early, the head may get stuck at this stage, and I believe fully that this is what we are seeing in the vast majority of cases of long, difficult second stage.
So, what happens if we wait, and the baby makes the internal rotation?
Well, in the majority of cases, unless the woman’s midpelvis and/or pelvic outlet (the space between her ischial spines, and the space between the pubic bone and coccyx and ischial tuberosities) is truly too tight a fit, the baby will naturally slip down that next level, past the spines, and fully drop onto the pelvic floor musculature. This sling of muscle, mind you, also contains both sympathetic and parasympathetic nerves, as well as pressure and stretch receptors, all of which do a wonderful dance, causing signals to the brain which cause a cascade of hormonal response.
The sympathetic nerves and hormonal response causes a sudden rush of adrenaline to the womban (and her baby gets one also), meanwhile the parasympathetic induces another rush of oxytocin (the hormone of uterine contractions and of loving bonding). All these nerves and subsequent responses in the brain and body are responsible for a profound physiologic shift, which causes the FER. Big waves of contractions begin again after likely having paused for a bit prior, the uterus but also entire body bears down in a powerful way, and the woman works to hold this freight train of energy with gentleness through her breath, breathing that baby out.
What I think we need to understand, however, and what has somehow become my mission, is the understanding of what makes this mechanism sometimes go a little less than full force and instantaneously.
The biggest factor in this nuance of experience is in the particularities of an individual’s pelvic floor musculature and the nerve force in those nerves. In other words, is the baby’s head able to truly rest evenly on the sling of muscles and nerves, thus sending a healthy nerve response to the brain? And, in turn, is that nerve tissue able to carry a strong signal, not impinged by imbalance, adhesions or tension in the muscles?
This is a complex subject to delve into, with more nuances that will require a deep dive in my courses, but the foundation of understanding is crucial here: womben are going to need tailored care to address pelvic floor issues and neurological function if they have any issues that may be in the way of this healthy response. Not every womban will have issues, obviously, but for those who do, a combination of bodywork or self-care massage, and exercises, as taught in my online education portal, is essential.

Courting the Parasympathetic Vagus Nerve Response ~ The Wise Woman Path to Birth Without Pain or Fear
The feminine archetype is the domain of the parasympathetic.
She is receptive. She rests. She digests. She chooses the sperm from the place of consciously receiving, not by being dominated or succumbing.
She also does not simply shut down, freeze, dissociate… There is a healthy vagal response, not one which becomes all encompassing, causing contraction AWAY from life and challenging stimuli.
Of course, the healthy Womban is able to both activate when needed, and be in repose when desired.
Our culture as a whole has a large demographic of people living in perpetual sympathetic overdrive. We live in fight or flight, racing to the finish line… living in a strong masculine dominant drive which is not healthy even for males to set up shop in.
For the ancient masculine, warrior archetype (which yes, some women engaged in throughout prehistory as well), the sympathetic response was reserved for that quick flash of action in the hunt, or to defend, or even in times of greater expense such as battle.
But the battle must end, the hunt resolve, and hopefully either scene will end with a feast. Rest, and digest.
The feminine, and the masculine in the pre-hunt pursuit/stalking phase, exists in a deeper brainwave state, predominated by the parasympathetic, primarily mitigated by the vagus nerve.
Of course, we also have a parasympathetic branch in the pelvis, and for the womb, it is particularly crucial to maintain a healthy response in this area as well. This quite literally allows us to root in to the Mother and have a healthy sacral response, that push/pull that comes from our electromagnetic connection to the Earth herself. This is the true source of instinct and even what some may consider intuition.
Modern medicine would list the pelvic splanchnic nerves as primarily nerves of communication between pelvic viscera and brain, having a role in the hormonal cascade of birth and beyond. What we often overlook is the importance of the healthy response of all nerve fibers, including autonomic, and sensory nerves, which can be dampened or deadened by trauma, physical restriction, or lesions of the nerves themselves. The pelvic nerves are a subject for an entire story all their own.
But the primary focus of parasympathetic activation is in the role of the vagus. This article is going to get rather intellectual here, but bear with me, because at the end, I’m going to tie it in for you with the world of physiologically normal birth, and I want you to get this… I truly do believe this nerve, and our nervous system as a whole, deserves our attention and some contemplation.
In India, they have long understood the role of this two-branched 10th cranial nerve which they called Ida and Pingala, the lunar and solar channels. They understood what we are now only beginning to understand about the importance of these nerves on the spiritual foundation for our growth as human beings. They show these nerves as if they were two serpents, crossing at the chakras, or energy centers, and meeting at the third eye, in the brain, where their consciousness can merge with the energy of the Susumna or central channel (the spinal cord) in order to open the Crown chakra. A lot of yogic study and inquiry goes into the activation of these three primary channels, and balancing their energies in the body.
While the connection remains somewhat nebulous, there is some relative mapping of the left and right vagus nerves (Ida and Pingala) and their relation to the anterior (front/ventral) and posterior (back/dorsal) portions of the vagus’ pathway. This is the modern concept created by Dr Steven Porges and Peter Levine call polyvagal theory, the understanding that the dorsal branch and ventral branch of the vagus act in somewhat different ways.
To put it simply, the dorsal (back) vagus is our more primitive vagal nerve, common to all animals including fish. Its response is responding to cues in a way which pulls us away from connection, out of awareness, and into a state of self-protection. It is the root of the “freeze” response. It can come in so strongly to counteract sympathetic arousal, that it can lead to dissociation, collapse, or the inability to think or emote clearly.
Typically, the dorsal vagus serves to help the body pendulate between activation and relaxation. But when it is trying to counteract an overactive sympathetic response, it can shut us down. In other words, it can be a trauma response.
Meanwhile the ventral (front) vagus is a newer addition that is found in mammals but not reptiles, birds or fish. Its response is to respond to cues by connecting and activating socially, fostering emotional safety and connection. This part of the vagus nerve system is predominated by the nerve’s pathway in the face and throat, relating to communication and social action/ engagement and self-expression. When we respond in a healthy way to stimuli, even challenge, we are able to activate fully into our healthy social engagement and proper attachment/bonding behavior. In other words, we are able to meet life and other beings even in difficult conversation where they are at, rather than fighting, fleeing, or freezing/dissociating.
To my best understanding, interestingly, the right branch of the vagus (the Pingala or Solar channel) runs to the front in the neck region, supplying these parasympathetic vagus nerve fibers to the larynx and pharynx, the organs of our expression. From there however, it is actually the left vagus nerve, the Ida/Lunar which travels through the anterior part of our thorax (abdomen), while the Solar channel continues along our back.
My theory of this is that this Yang energy of the Solar channel is more closely correlated to the motor nerves of the central nervous system in this region of the solar plexus chakra. Our soft belly, while theoretically the realm of outward action, is actually the more receptive side of this thoracolumbar region. That’s my best way of relating to this polyvagal theory anyway, and it certainly tracks well with my sentiments about the particular receptivity of the anterior of our body in this region to other people’s energy, despite the front side of our body generally being the domain of forward momentum and outward expression of will.
The vagus wanders from the medulla oblongata, down either side of the neck, wrapping itself around the heart, other organs, and trailing along the mesentery into the majority of the gut, sending fibers of its energy of repose (restfulness) into our very visceral response.
There, it meets the sacral parasympathetic branches of the pelvic splanchnic nerves, not directly touching of course, but dancing their dance of parasympathetic response in the space occupied by our womb, our iliopsoas muscles, and our gut.
We have to remember also, this is not a one way street, but rather, the nerves receive information in the form of pressure sensation, and carry impulses back to the brain which opens a hormone cascade. This is an important part of giving birth, and it’s also an integral part of courting the body’s capacity for balance.
So what does polyvagal theory have to do with the way womben, and those generally attuned to the feminine magnetic polarity, make decisions, the way we walk in the world?
The wounded feminine is in direct opposition to the wounded masculine. He dominates, is in perpetual war, constantly courting the sympathetic response, until He burns out, sometimes too late in the game after wars have decimated communities.
Meanwhile She collapses, involuting into a vacuum of dorsal vagal dominant freeze response. She fawns. She freezes. She encapsulates. She becomes a mess of adrenal fatigue and poor hormonal balance. Her grief crusts around her like the salt from the ocean which, ironically may be homeopathically part of her healing picture.
She fears social connection, or she fears conflict in connection, and thus is unable to do the real work of relating, which requires a give and take, and conflict resolution skill.
She becomes an island, attempting to do it alone, attempting to stand without community, even while she claims to desire this connection and safety net. She tends to push away that which she seeks, subconsciously, through subtle programs of sabotage, or through subtle or not subtle victim mentality.
Her very self protection becomes her undoing because it creates a distancing from the very medicine she needs. Community. Co-creation. Collaboration.
For the masculine side to be healthy and vital, we must de-stress our entire system, releasing the need to control and willfully bend fate to our personal desires. This isn’t to say that we give up on taking action entirely, but instead we marry our will to the desire for the good of our entire community. We recognize that only that which truly serves the whole, will serve us in our highest iteration.
For the feminine to be healthy and vital, she must build a healthy social response, releasing the collapse into excessive waiting, receptivity, inaction, and perhaps even victimization. She must learn to lean INTO conflict, rather than away, and how to discern true danger, from a perceived danger from an overly flighty or dissociative nervous system response.
Even in our self-preservation response of isolation, we lean away from a truly healthy and balanced parasympathetic response. What we are finding is that the parasympathetic actually responds faster than the sympathetic- milliseconds rather than seconds- allowing us to foster a deeply nourishing social activation response that allows us to find our true root in the Whole.
Through this response, we are able to more quickly respond to life, easily moving between active and passive states… between higher and deeper brainwave states. This is the fluidity that is the true domain of the feminine. The electromagnetic pulsation of the Earth herself, and likewise of our own crystalline electromagnetic bodies. We are meant to pulse. Active, passive, active, passive… with ease and grace.
The wounds of the feminine push us often into sympathetic overdrive and eventual dorsal vagal collapse. For many, the healing crisis then begins with an activation back into sympathetic, un-crusting that grief wound, finding her fire, pumping air and blood heat back into her horrendously dampened system. But she cannot remain there, either, or she will only collapse again, often pushing away her allies in the process, or alienating herself.
What she must do is court a healthy ventral vagal response, and learn to mitigate the two. Fire and Water, self and community, in a dance of wholeness.
Her medicine is in stepping out and realizing she was never meant to be an island. Our very societal fabric is woven from these threads of sympathetic nerves of entire populations of people caught in fight or flight. Our dog eat dog, man eat man world of “pick yourself up by your bootstraps” mentality was not created for safe social interaction. Of course the feminine eventually collapsed here. Of course she built an egg shell of protection, encased in mineral deposits which could give her soft belly a break from harsh realities.
But the medicine must be found none the less, not in forging a new path as a solo, masculine, entrepreneurial business woman of the modern age…
Her true medicine lies in her ability to story tell while weaving threads of polyvagal response, Sun AND moon threads, with her sisters around the collective loom. Many hands make light work, and together the feminine matriarchal archetype can rise again, courting the response of the deep repose alongside healthy social response… lunar receptivity and solar activity… the kind that does not burn like a wildfire blazing across the lands as the fiery sympathetic does… but instead the kind of heat which gently warms us from afar.
Our collective initiation right now calls us to healthy community. Setting down the reins altogether and learning to pick up the threads instead and weave. Let the horses run free. Gather as humans again on our own two feet, on our haunches, and babble in circle, telling stories of Sun gods and Moon goddesses while we weave their stories into our tapestries, wearing them proudly.
The womben sat and gathered, cooked, chatted and story wove while spinning and weaving.
They did not have businesses. They did not hunt for the next client. People came to the wise womban’s hut for healing or to seek her midwifing because they knew that she would be there, holding the circle together with the other womben, just existing in the repose that knows her own Source.
And from there, she acts.
“The midwife performs her work by doing nothing. She teaches without speaking a word. Things arise and she lets them come. Things leave and she lets them go. Creating, not possessing. Working, but laying no claim. And when her work is done, she releases it. And so it lasts forever. “
~Whapio, in her Wise Woman re-iteration from the Tao de Ching
